Safety Pilot Landmark Accidents: Into the Abyss<br>
Why black hole approaches have bad reputations<br>
"Black hole" approaches describe runways that have no lights surrounding the airport and thus are susceptible to pilot misjudgment on height above the ground. They have been the destination for many an accident flight. Additionally, it's always instructive to look at how small details turn out to be factors and how they connect to form the accident chain. Links that have been present on many previous flights but never mattered before sometimes have a way of coming together to create a nasty outcome. A night visual approach made by a Federal Express Boeing 727 was all in a normal night's work, but the result was anything but routine.
The three-person crew reported for the scheduled flight to Tallahassee Regional Airport at FedEx's Memphis hub prior to 3 a.m., and the flight pushed back at 4:24 a.m. (Eastern Daylight Time). The first officer (FO) flew while the captain performed the pilot-not-flying duties. The flight proceeded uneventfully, and at 5:11 a.m., the flight engineer received the Tallahassee weather from Gainesville Flight Service, which indicated scattered clouds at 100 feet, 18,000 feet, and 25,000 feet; wind from 120 degrees at 5 knots; visibility 9 statute miles; temperature and dew point 22 degrees Celsius; and altimeter setting 30.10.
Which way?
The crew discussed which runway to use at Tallahassee, since both the tower and tracon were closed, and the captain decided on Runway 27. Atlanta Center instructed the flight to begin descent at pilot's discretion. At 5:16 a.m. the crew conferred on the weather and the FO began the approach briefing for Runway 27, "We'll plan on a visual to Runway 27. We'll back it up with this ILS Runway 27 full procedure, 272 [bearing in degrees] is the final approach course inbound...."
The FO continued, "Runway's 8,000 [feet long], plan on rollin' out to the end, got a PAPI on the left-hand side, pilot-controlled lighting, so if you can click it seven times, I'd appreciate it." So far, every thing was exactly as it should have been with the crew configuring themselves and the Boeing for the approach.
Color Vision and FAA WaiversBy Gary CrumpAn unknown color vision deficiency may catch new student pilots by surprise when they visit their aviation medical examiner for the first FAA medical exam. Although color deficiency is primarily a hereditary trait that's present in about 8 to 10 percent of the male population (and only about 0.5 percent in females), the deficiency can also be acquired later in life because of disease, eye trauma, or exposure to toxic agents. Color vision deficiencies occur in varying degrees of severity, and people with a deficiency who don't know they have it or to what degree perceive whatever colors they see to be "correct." With the advent of the glass cockpit in general aviation's technologically advanced aircraft (TAA) and the associated color cues on the displays, it's that variability and incorrect color perception that makes color vision requirements necessary for all classes of medical certification. However, there are several different FAA testing procedures available that can help determine the degree and type of color vision deficiency. Most aviation medical examiners (AMEs) use one of the pseudoisochromatic plates (PIP) tests for FAA physical examinations. PIPs are a series of small colored circles within a larger circle. The small circles are designed in different color shades to form specific characters or numbers that will appear different to color-normal versus color-deficient individuals. The Ishihara PIP test is often used by AMEs and is a highly sensitive test that identifies all color deficiencies, regardless of degree, so persons with even a very mild degree of color vision deficiency will likely not pass the Ishihara test. If you fail the color vision test, the AME still may issue you a medical certificate, but with a restriction that prevents night flying or use of color signal control (tower light gun signals).It's possible, though, to have that restriction removed by successfully completing one of the FAA-allowed alternative color vision tests. These tests include other types of PIPs, as well as several Lantern tests that project different colored lights. When the FAA has accepted the results of the alternate test, you will be issued a "letter of evidence" and a new medical certificate that has no night flying restriction. At each medical renewal, just have the letter available to the AME to avoid having the restriction reinstated on your next medical certificate when you again fail the color vision test in the office. Gary Crump is the AOPA medical certification director. |
But then, the FO asked the captain, "You wanna land on [Runway] Nine if we see it? We got a PAPI on Nine, too." The captain responded, "Yeah, maybe be a longer taxi for us, but way we're comin' in.... probably [Runway] Two-Seven be about as easy as any of 'em." The FO agreed, and the crew began the in-range check to configure the aircraft.
After several frequency changes, the Jacksonville Center controller advised the crew to expect a visual approach and to report the airport in sight. The captain then seemingly changed his mind and said to the FO, "Runway Nine, PAPI on the left side. I don't know.... You wanna try for Nine?"
The FO responded, "We're pointed in the right direction. I don't know, like you said, kinda a long taxi back." The captain said, "Yeah, that'd be all right." The FO continued, "I always thought you were supposed to land with the prevailing wind at an uncontrolled...." And the captain responded, "Well, at five knots, it's really the only advantage you have. Landing to the west you have the glideslope, which you don't have to the east."
The flight engineer asked the captain and FO whether they were ready to perform the approach checklist. At 5:28 a.m. the FO asked, "We ever decide if we're goin' [Runway] Nine or Two-Seven?" The captain responded, "Yeah, we can do Nine if you want to."The FO replied, "Okay, Runway Nine, visual, Runway Nine PAPI on the left side."
At 5:30 a.m., the captain advised the controller that they had the airport in sight, and the Boeing was cleared for the visual approach for Runway 9. The captain announced on the common traffic advisory frequency (CTAF), since the control tower was closed at the early hour, "Tallahassee, FedEx fourteen-seventy-eight, uh, extended, uh, left base leg for Runway Nine." The FO called for flaps and at 5:32:34 said, "I hope I'm lookin' in the right spot here." The captain responded, "See that group of bright lights kinda to the south down there and you see the beacon in the middle of it? Right over there. You're kinda on about a ten-mile left base or so...." The FO said that he'd been looking at the wrong flashing light and had mistaken it for the airport beacon.
Into the abyss
At this point there was some further discussion about the pilot-controlled lighting; the aircraft microphone was keyed five times to activate the lights at 5:34:26, and at 5:34:35 the captain said, "There we go." The FO called for additional flaps and landing gear, and at 5:35:42, the captain advised on the CTAF that Flight 1478 was turning onto final for Runway 9. The crew then ran the final before-landing checklist.
At 5:36:20 the ground proximity warning system (GPWS) announced that the airplane passed through 1,000 feet agl. At 5:36:37, the 727 was transitioning from an angled base-to-final leg to line up with the runway about 2.5 nautical miles from the airport.
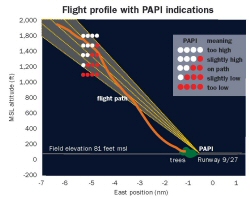
The role of the runway visual guidance system (precision approach path indicator [PAPI]) was about to become critical. The approach into Runway 9 at Tallahassee is over an unlit forest and is described as a "black hole" approach. There is no good visual reference from the surrounding lights, terrain, or electronic vertical guidance from an instrument landing system (ILS) or global positioning system (GPS). The pilot was totally dependent on the PAPI to maintain a safe glide path.
The NTSB's performance study indicated that the PAPI would have displayed one white light and three red lights when viewed from the cockpit as the Boeing turned onto final approach. This means the aircraft was somewhat below the desired path and needed to climb or at least stop descent. At 5:36:40, the PAPI display would have shown four red lights, indicating that the aircraft was well below the safe vertical path. (The illustration below shows the airplane's descent profile in relation to the PAPI light indications, the runway, and treetops.) The aircraft at this point was less than 800 feet agl and about 2.8 nm from the runway. It never intercepted the proper glide path but stayed in the danger zone for the rest of the approach.
The power on the three engines momentarily increased from about 1.05 to 1.24 engine pressure ratio (EPR) and then decreased to 1.17 EPR. At 5:36:43, as the airplane approached 500 feet, the captain offered to set the flaps to 30 degrees, and the FO responded, "Please." At 5:36:47 the GPWS announced that the airplane was passing through 500 feet agl, and just a few seconds later the captain noted that the approach was "stable." The NTSB's evidence positioned the airplane 1.8 nm west of Runway 9 on final approach, descending through 500 feet agl, with a vertical speed of 1,248 feet per minute (fpm), engine power settings of about 1.17 EPR, and an airspeed of 152 knots. The normal power setting for the aircraft in this configuration was noted to be 1.3 to 1.45 EPR. The investigation noted that the highest rate of descent during the later stages of the approach exceeded 1,400 feet per minute. The normal vertical speed on a three-degree glide path at 140 knots is about 750 fpm. It is a mandatory call-out for the pilot not flying when the descent rate exceeds 1,000 fpm on short final. The approach was anything but "stable." At 500 feet, according to FedEx procedures, the crew should have abandoned the approach under these conditions.
At 5:36:49 a.m., the FO said, "I'm gonna have to stay just a little bit higher. I'm gonna lose the end of the runway."The captain responded, "Yeah, yeah, OK." At 5:36:52, the flight engineer asked, "Flaps?" and the captain responded, "Thirty, thirty, green light," referring to flaps, and the flight engineer asked, "Landing clearance?" The captain responded, "Clear to land Runway Nine."
At 5:36:58 the engine power began to increase from 1.17 EPR, reaching 1.20 EPR about four seconds later. At 5:36:59, the captain advised Tallahassee traffic that Flight 1478 was on short final for Runway 9. At 5:37:09, the captain said, "It's startin' to disappear in there a little bit, isn't it?" This was a possible reference to the end of the runway and the fact that the Boeing was so low that trees were now blocking a clear view of the threshold or that there were some scattered clouds blocking the view.
Controlled flight into trees
The Boeing was now 0.9 nm west of Runway 9, descending through 200 feet agl with a vertical speed of 528 fpm at 146 knots. The PAPI indication would have been four red lights. At 5:37:13 the flight engineer declared that the before-landing checklist was complete. At 5:37:14, the GPWS announced that the airplane was 100 feet agl; during the next several seconds the descent profile was steady but the engines were spooling up, perhaps in recognition that the aircraft was about to land short. At 5:37:20, the cockpit voice recorder (CVR) recorded the sound of a crunch, and at 5:37:21, the GPWS announced 30 feet agl. About 5:37:22, the CVR recorded another crunch sound, and the number one engine EPR began to increase rapidly.
The 727 descended into trees in a right-wing-low, slightly nose-up attitude, and rotated 170 degrees, coming to rest on a heading of 260 degrees, 1,556 feet west-southwest of the runway. A post-impact fire ensued, and the aircraft was destroyed, but the crew escaped through the captain's sliding cockpit window before the fire reached the front of the aircraft. It was one hour and 14 minutes before sunrise.
In reviewing the crew's experience, the NTSB also recorded its flight schedule in detail on the days preceding the day of the accident, July 26. It's worth understanding the trip schedule; all times are local times.
The captain — pilot not flying
The 55-year-old captain held an airline transport pilot (ATP) certificate and multiple type ratings with total flight time in excess of 13,000 hours, with 2,754 hours as a Boeing 727 crew-member and 861 hours as a 727 pilot in command. He held a current first class medical certificate with the only restriction requiring that he wear glasses. All his proficiency checks were satisfactory with company training in visual approaches, non-towered airport operations, fatigue management, and crew resource management, but he had not seen FedEx's black hole or controlled flight into terrain (CFIT) training modules.
The captain stated that he was healthy and did not take prescription medications or smoke and that he drank alcohol only occasionally. The captain's normal rest hours when not flying were between 10 p.m. and 7 a.m.
The captain did not sleep well the night of July 24: He reported being awake for a couple of hours to take care of the family dog, which was in deteriorating health. He slept on the couch to care for the dog during the night and got up three times. He awoke about 7:30 a.m. on July 25, 2002, and described his sleep quality as "marginal, not really good." He stated that he slept from about 9 p.m. on July 25 to about 12:30 a.m. on July 26; he described his sleep during that 3.5 hours as "pretty good" and said that he did not feel fatigued when he arrived at Memphis for the accident flight.
The first officer — pilot flying
The FO, age 44, held an ATP and a flight engineer certificate for turbojet-powered airplanes. The most recent FAA first-class medical certificate was issued on October 9, 2001, with no restrictions or limitations but with a statement of demonstrated ability (SODA) for defective color vision. The medical certificate and SODA were issued on the basis of previous operational experience as a career Navy pilot with more than 5,000 hours in P-3s. Total flight time was in excess of 7,500 hours, including 1,983 flight hours as a 727 flight crewmember and about 526 hours as a 727 second in command.
The FO felt the reserve schedule he worked was difficult because the sleep-wake cycle was frequently changing. Follow his schedule to get an idea of the shifting nature of a reserve pilot's life: On July 23, 2002, the FO departed Memphis at 3:30 a.m., flew to Dulles International Airport in Washington, D.C., then to Greater Rochester International Airport in New York, and arrived back at Memphis at 11 a.m. He went to an apartment leased with other FedEx pilots, fell asleep at 11:30 a.m., woke for dinner, returned to the apartment, and slept through the night.
The FO awoke again on the morning of July 24 and engaged in routine activities around the apartment. According to a roommate, the FO complained about the reserve schedule he was flying because it reversed day and night sleeping on consecutive days. He retired about 9 p.m. and slept until early morning on July 25 to report for duty at 3 a.m. on a flight to Winnipeg International Airport in Manitoba, Canada, arriving at 6:45 a.m. He slept at a hotel for about five to six hours and reported for duty at Winnipeg again at 6:20 p.m. His next flight arrived at Grand Forks International Airport in North Dakota at 7:35 p.m. and departed Grand Forks at 8:57 p.m. to arrive in Memphis at 11:03 p.m.
After the Grand Forks flight landed, the FO was notified that he was scheduled to work Flight 1478 (the accident flight) to Tallahassee, which was scheduled to depart Memphis about four hours later. The FO accepted the trip, noting that it did not violate existing pilot union agreements and would not result in exceeding flight and duty limits. He slept for about 1.5 hours in a private sleep room in FedEx's crew rest facilities at Memphis before he met the captain to prepare for the accident flight.
Red is red
In a peculiar twist to this accident, where the PAPI played such an obvious part, accident investigators wanted to know whether the FO could distinguish between red and white, especially because he had a SODA that allowed him to fly with a color deficiency.
According to the FO's Navy medical reports, he consistently demonstrated 20/20 or better near and distant visual acuity in both eyes without correction during his 16 years of Naval service. Color vision testing was performed by means of the Farnsworth Lantern (FALANT) test (the Navy's primary color vision screen), and the FO consistently passed. However, during a July 24, 1995, evaluation for an FAA medical certificate he did not pass a color vision screen that was conducted using pseudoisochromatic plates. (These are colored numbers buried in contrasting colored dots that are typically used for civilian medical certification.)
The FO's FAA-designated medical examiner contacted the FAA's regional flight surgeon for advice and was told to issue the medical certificate with a SODA for the color vision deficiency based on his successful flight experience to this point. Correspondence between the doctors indicated a color vision loss suggesting a "mild red-green defect." The FO told investigators that he never experienced any difficulty distinguishing red and white on PAPI or visual approach slope indicator (VASI) lights.
The flight engineer
The flight engineer, age 33, held an ATP certificate with a multiengine land rating and a flight engineer rating for turbojet-powered airplanes. He had 2,600 total flight hours and 346 hours as a 727 flight engineer.
The flight engineer normally slept between 10:30 p.m. and 6:30 a.m. On July 23, 2002, he awoke around 9 a.m. He went to bed about 10 p.m. When he awoke about 8 a.m. on July 24, he went boating with his children from about 9 a.m. to about 11 a.m., took a nap from about 1 p.m. to about 3:30 p.m., and engaged in routine activities at home until it was time to travel to his duty station (Memphis). He arrived at the airport in Albany, New York, about 10 p.m. to ride on a flight to Memphis. He stated that he napped for about 30 minutes during the commute to Memphis, arriving at Memphis about 11:30 p.m. The engineer then slept another 90 minutes in FedEx's crew rest facility at Memphis before reporting for duty at 2:48 a.m. on July 25.
His flight departed Memphis at 3:58 a.m. on July 25 and arrived at Buffalo Airport in New York at 5:58 a.m. The flight then departed Buffalo at 6:26 a.m. and arrived at Ottawa International Airport in Ottawa, Canada, at 7:14 a.m. The flight engineer checked into a hotel and slept about six and one-half hours. Upon awakening he was notified of his assignment to Flight 1478 to Tallahassee on July 26. He stayed at the hotel and returned to the airport at 6:06 p.m. on July 25. His flight departed Ottawa about 9:39 p.m. and arrived at Memphis at 11:59 p.m. The flight engineer arrived at Memphis around midnight, had his fingerprints taken to satisfy a new security policy, and then relaxed in a recliner chair for 30 to 60 minutes. He began preparing for Flight 1478 about 1:35 a.m.
Airport factors
FedEx provides its flight crews with additional information to augment the published Jeppesen airport and approach charts for Tallahassee. These pages include airport-specific precautions, control tower hours of operation, noise abatement procedures, weather information, and runway lighting/traffic advisory information for hours of non-tower operation. FedEx characterized the CFIT risk at Tallahassee as "moderate" stating, "Local ATC [air traffic control] and radar coverage unavailable at certain times. ILS not installed in all directions, potential non-precision approach...."
Runway 9 was equipped with high-intensity runway lights, in-pavement runway centerline lights, and runway end identifier lights. A four-box PAPI light system was located on the left side of Runway 9 to provide lighted signal glide path guidance relative to the published 3-degree glide path to the runway's touchdown zone. As previously mentioned, pilots must activate the lighting on the CTAF. When triggered, all lights (including PAPIs) turn on and remain lit for 15 minutes. The airport lighting activation log recorded the lights were triggered at 5:34:26 a.m. and the runway lights were set to medium intensity.
In PAPI operation, four lights are aligned perpendicular to and about 1,000 feet from the approach end of the runway. An optical apparatus splits the lamp beams horizontally into red (lower) and white (upper) beams. When an aircraft is on a 3-degree glide path, two white lights and two red lights appear. If the aircraft is too high, the lights are all white, and if it is too low, they are all red. If the aircraft is slightly high, three white lights and one red light appear, and if it is slightly low, three red lights and one white light appear. The PAPI was checked for alignment and operation subsequent to the accident and found to be operating normally.
Discussion
It's very clear what happened in the accident — the crew allowed the aircraft to get too low on the approach — but "the why" has multiple factors that most of us can relate to. The system of cross- checks that keeps aviation as safe as it is broke down. Balancing convenience and safety is something that pilots do on every flight, and while no one ever deliberately takes a shortcut to save time at the expense of safety, unseen factors sometimes creep into the equation.
The captain originally decided on Runway 27 with the ILS and then changed his mind, perhaps thinking that they might save a few minutes and that the prevailing wind ever so slightly favored Runway 9. Abandoning an ILS at night even in visual conditions should never be done casually. The PAPIs were assumed to suffice, but the captain didn't see red or at least do anything to intervene. His comment regarding the stability of the approach while the aircraft was in a high sink rate on short final is curious.
The FO, as the pilot flying, obviously did not heed the PAPI, assuming he could interpret it with his color deficiency. Additionally, he did not have the aircraft power equation right. A high sink rate and low power setting pretty much ensure a short arrival.
The flight engineer, a third set of eyes in the cockpit, was apparently distracted by his other duties and failed to mention either the discrepancy on the visual glide path or the non-stable approach condition.
The crew's schedule is a big factor and a political hot potato. For decades professional pilot associations have argued that companies demand too much from crews while companies argue that they and the FAA have shown through millions of flight hours and successfully completed flights that fatigue is not a safety issue.
My take is that at least two-thirds of this crew was suffering from chronic fatigue (the captain and the FO). They were not awake enough to catch all of the factors that made up this accident chain.
Most of us have flown when truly tired and made lots of mistakes. Usually another pilot, in the case of crewed aircraft, or luck, in the case of single-pilot operations, bails us out. Sometimes ATC catches the error, but no controller was on duty in this situation.
For light general aviation pilots the lessons learned are: Use electronic approach guidance at night whenever it is available. That includes ILS and Wide Area Augmentation System (WAAS) GPS approaches. Use IFR procedures even in visual night conditions. Long, well-lit runways are far superior to short ones. Some of the airports I flew to when I was younger were so marginal for the conditions that I'm fortunate to be writing this article. Obviously, adhere to PAPIs and the like. If you have a SODA because of color deficiency, be careful about depending on it for night visual approaches, and, finally, be keenly aware that fatigue can deactivate your normal good judgment without any warning.
The NTSB spent considerable time in the report discussing the FO's color deficiency, but this FO had 20 years of flight time and literally thousands of hours of successful flights. In my opinion, fatigue was the big player in the FO's failure to fly the approach properly and notice the PAPI. After all, there were two other pilots with normal color vision who missed it also.
In conclusion
"The National Transportation Safety Board determines that the probable cause of the accident was the captain's and first officer's failure to establish and maintain a proper glide path during the night visual approach to landing. Contributing to the accident was a combination of the captain's and first officer's fatigue, the captain's and first officer's failure to adhere to company flight procedures, the captain's and flight engineer's failure to monitor the approach, and the first officer's color vision deficiency."
Related Articles


